35 year female with c/c SOB fever generalised weakness
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
Case :
35 years old female,resident of choutuppal,occupation cleaning works in the hotel, came with chief complaints
SOB since 3 months ,
fever since 3 months ,
generalised weakness since 1 month.
HOPI:
Patient was apparently asymptomatic 3 months back then she had shortness of breath which relieved on taking rest ,No orthopnea, no PND.aggravated by prolonged walking
-C/o generalised weakness since 1month ,2 weeks back she went to the Suryapet hospital ,there they did haemogram and diagnosed as anemia, at that time her hb was 3 gm/dl.
-C/o fever since 1 month, intermittent in nature.10 days back she had high grade fever,relieved on taking medication ( Dolo625mg )
-C/o cough since 2 days ,which is productive, yellowish in colour and non foul smelling.
-H/o heavy bleeding last month (lasted for 11 days(1st 6 days heavy bleeding then next 2 days bleeding is stopped then again 5 days bleeding occured)
-No H/o blood in the stools, hematemesis , Malena,hemoptysis.
MENSTRUAL HISTORY:
-Regular cycle ,with normal flow until last Feb.
-Last month (March)heavy bleeding without clots ,lasted for 11 days (1st 6 days heavy bleeding then next 2 days bleeding is stopped then again 5 days bleeding occured)
DAILY ROUTINE:
She wakes up at 6 am and does her morning routine and drinks tea at 9 :am,(she does not eats breakfast) and goes to work (works in hotel) ,lunch at 3 pm ,again continues work and comes back at 6 pm ,dinner at 8 pm (sometimes she eats, sometimes will sleep without eating dinner only) , goes to bed at 10pm.
PAST HISTORY:
Not a k/c/o Diabetes,asthma, coronary artery diseases,epilepsy,thyroid disorders.
FAMILY HISTORY :
Not signigicant
PERSONAL HISTORY:
Diet- mixed
Appetite - normal
Sleep -normal
Bowel and bladder -regular
Addictions- none
GENERAL EXAMINATION:-
-Patient is conscious, cooperative, with slurred speech
Well oriented to time, place and person
-thinly built and malnourished.
Pallor - present

Icterus - absent
Clubbing - absent
Cyanosis - absent
Lymphadenopathy- absent
Edema - absent
Koilonycia- present

VITALS:
Temp:97.8°F
B.P:110/70 mmhg
P.R:82 bpm
R.R: 20 cpm
SYSTEMIC EXAMINATION:
CARDIOVASCULAR SYSTEM:
Inspection :
Shape of chest- elliptical
No engorged veins, scars, visible pulsations
JVP - raised
Palpation :
Apex beat can be palpable in 5th inter costal space
No thrills and parasternal heaves can be felt
Auscultation :
S1,S2 are heard
no murmurs
RESPIRATORY SYSTEM:
Inspection:
Shape- elliptical
B/L symmetrical ,
Both sides moving equally with respiration .
No scars, sinuses, engorged veins, pulsations
Palpation:
Trachea - central
Expansion of chest is symmetrical.
Vocal fremitus - normal
Percussion: resonant bilaterally
Auscultation:
bilateral air entry present. Normal vesicular breath sounds heard.
Investigations :





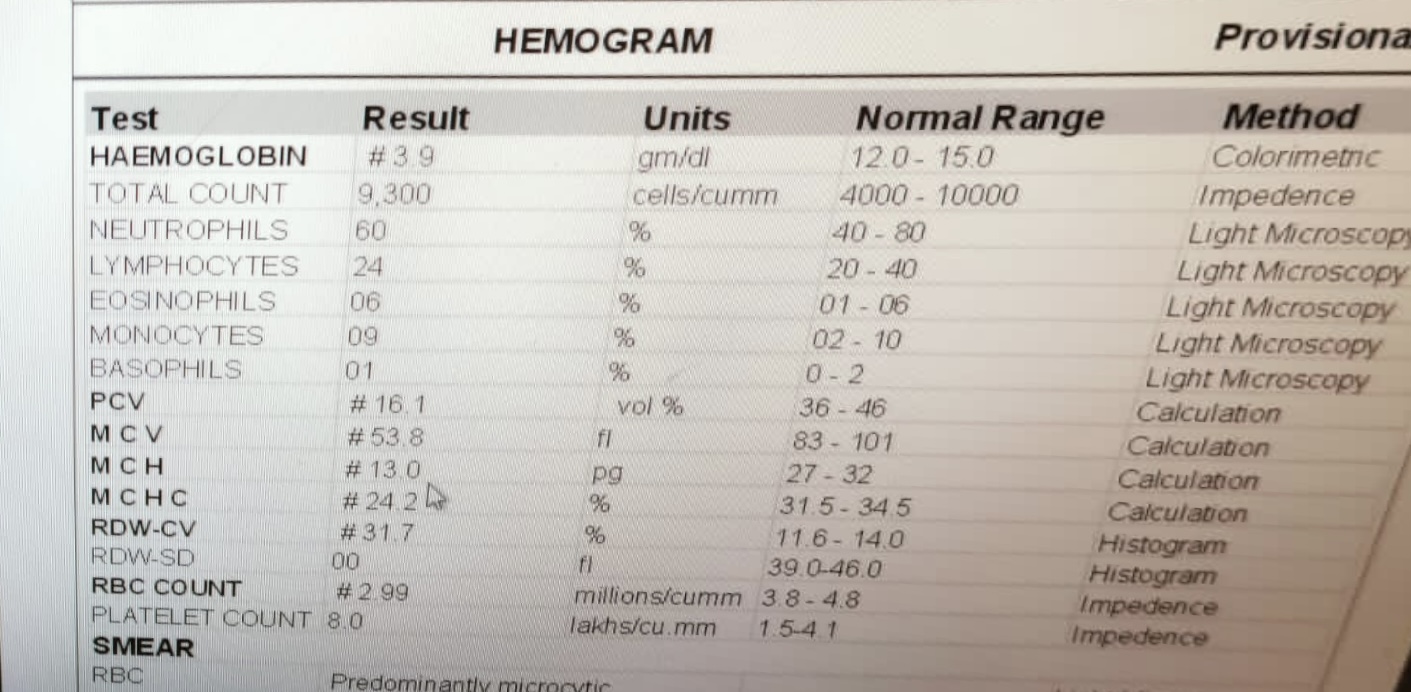





Charts:

PROVISIONAL DIAGNOSIS:
Anemia secondary to menorrhagia
Treatment
Tab paracetamol
Tab Ferrous Ascorbate & Folic Acid

Comments
Post a Comment